In vitro fertilization (IVF) refers to a procedure designed to overcome infertility and produce a pregnancy as a direct result of the intervention. In general, the ovaries are stimulated by a combination of fertility medications and then one or more oocyte(s) are aspirated from ovarian follicles. These are fertilized in the laboratory ("in vitro"), after which, one or more embryo(s) are transferred into the uterine cavity.
A complete infertility evaluation is performed on both partners prior to embarking on IVF.
Causes of infertility:
Tubal factor (IVF is primary therapy if tubes are completely blocked)
Severe male factor infertility (mild male factor may be treated with inseminations; if male factor is severe, IVF is primary therapy of choice)
Diminished ovarian reserve (time to conception is critical and success with other therapies is low)
All other causes of infertility, after failing treatment with less invasive therapies (eg, ovulatory dysfunction, endometriosis, unexplained infertility)
Ovarian failure (donor eggs need be used in this case)
In young women, treatable causes of subfertility are treated prior to initiating IVF because treatment may enhance the likelihood of natural conception.
In general, in the absence of absolute impediments for conception (blocked fallopian tubes, severe male factor), couples may be offered three to six cycles of superovulation and intrauterine insemination (IUI) before proceeding to IVF.
IVF has also been used to achieve pregnancy in gestational carriers of women who do not have a uterus or in whom pregnancy is medically contraindicated.
Who should be treated with in vitro fertilization?
IVF can be used as an effective treatment for infertility of all causes except for women with infertility caused by an anatomic problem with the uterus, such as devere intrauterine adhesions.
It is generally used in couples who have failed to conceive after at least one year of trying who also have one or more of the following:
Blocking fallopian tubes or pelvic adhesions with distorted pelvic anatomy. Women that have had tubal ligation and are considering tubal reversal surgery as well as men that are considering vasectomy reversal surgery might also consider IVF.
Male factor infertility (low sperm count or low motility). ICSI is an IVF procedure that can fertilize eggs even with poor sperm quality.
Failed 2-4 cycles of ovarian stimulation with intrauterine insemination.
Advanced female age- over about 38 years of age. In vitro fertilization and advanced maternal age is discussed in detail on the female age page.
Reduced ovarian reserve, which means lower quantity(and sometimes quantity) of eggs. A day 3 FSH and estradiol test, antral follicle counts and AMH hormone levels are often done as screening tests for egg quantity and quality is usually treated with either IVF, or with IVF with egg donation.
Severe endometriosis.
Unexplained infertility when inseminations have failed. Unexplained infertility menas standard fertility tests have not found the cause of the fertility issue.
Pre-cycle factors associated with success
Several preprocedure factors can affect the success of IVF (age, infertility diagnosis, past reproductive-obstetrical history)
Younger maternal age there is age-dependent decline in fertility in older women, particularly those over 40 years.
Adequate ovarian reserve — Serum follicle stimulating hormone (FSH) and estradiol concentrations may help predict the success of the IVF procedure. A high day 3 level is a poor prognostic factor.
Absence of hydrosalpinges — Studies have consistently shown that the presence of a hydrosalpinx is associated with poor IVF outcome: the live birth rate is one-half that of women without hydrosalpinges
Factors with no or a negative effect on success
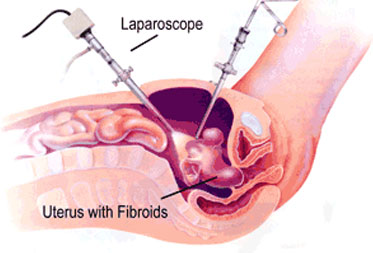
Leiomyoma — The effect of leiomyomas on IVF is dependent on their location: submucosal myomas decrease the chance of success, whereas subserosal myomas do not appear to have any effect.
Endometrioma — Whether an asymptomatic endometrioma should be removed prior to IVF is controversial; there is no consensus on the optimum approach. We do not routinely resect endometriomas prior to initiating IVF as surgery does not improve outcomes of ART and may damage ovarian reserve
Smoking
Previous pregnancy history — A previous live birth is associated with higher likelihood of successful IVF
Previous unsuccessful IVF cycle — Lack of success in an IVF cycle does not appreciably decrease success rates during subsequent treatment until approximately the fourth IVF cycle
Obesity — Infertility is more prevalent among overweight and obese women, and IVF may be slightly less successful in these women.
FOLLICLE ASPIRATION AND FERTILIZATION
Oocyte retrieval — Currently, oocyte retrieval is achieved almost exclusively by the transvaginal ultrasound-guided follicle aspiration method. It is performed 34 to 36 hours after hCG administration.
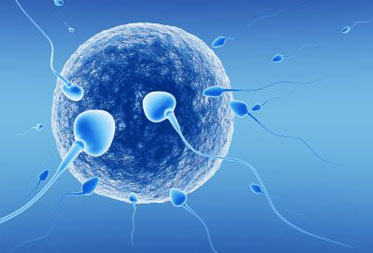
Fertilization in vitro — To achieve fertilization, recovered oocytes are mixed with spermatozoa in a small volume of culture medium.
EMBRYO MANAGEMENT— Fertilization of the oocyte is confirmed by observing two pronuclei within the zygote about 17 hours after insemination or ICSI. After fertilization, the individual cells of each embryo ("blastomeres") divide every 12 to 14 hours, so that the embryo reaches approximately 8 cells by 72 hours after egg retrieval. Embryos between days 2 and 4 are called "cleavage stage embryos." The blastocyst stage is reached by about day 5 after retrieval, and implantation is expected by day 7 after egg retrieval, so transfer should take place prior to this time.
Embryo transfer — After fertilization, embryos are maintained in culture for a variable period of time. Transfer embryos to the uterus about 72 hours after egg retrieval (four to eight cell, cleavage stage) there is a slight increase in pregnancy rates with day 3 versus day 2 transfer. The additional 24 hours in culture from day 2 to day 3 allows identification of embryos that stop dividing and thus are not viable. The live birth rate per transfer is generally higher with Day 5 than Day 3 transfer. Embryos can be inserted into the uterus using a catheter via the cervix.
The usual number of embryos transferred depends on a number of factors, including maternal age, the number of oocytes retrieved and availability of embryos for cryopreservation. . No more than two embryos should be transferred in young women. No more than three or four embryos be transferred in 38- and 39-year-olds. However, this is controversial, and some authors suggest transfer of no more than two embryos regardless of maternal age.
Luteal phase support — supplementation is generally initiated on the day of oocyte retrieval or at the time of embryo transfer.
Cryopreservation — Embryos in excess of those that can be safely transferred can be cryopreserved for future use.
FOLLOW-UP
Expected course — Post-transfer, the patient can resume her regular daily activities. Neither physical activity nor diet has been shown to have an impact upon the success of embryo implantation or conception.
Monitoring for pregnancy — first blood test is usually obtained no earlier than 12 days after egg retrieval, although some programs start testing later. HCG administration prior to oocyte retrieval results in serum hCG levels between 60 and 300 mIU/mL, but this hCG is generally completely cleared by two weeks after administration, which is about 12 days after retrieval, so it should not interfere with pregnancy testing.
The cause of infertility affects IVF outcome. Live birth rates are highest in women with ovulatory dysfunction and lowest in those with diminished ovarian reserve (40.4 versus 14.5 percent)
Pregnancy rate — On a per-cycle basis, because of the transfer of multiple embryos, the results of IVF treatment now exceed the fecundability of natural conception cycles in the general population (live births per natural cycle 27.7 percent, live births per artificial cycle 30 percent)
Reasons for failure — Failure can occur during any step in the IVF process, and often the reason for failure is not known. Follicles may not develop due to poor ovarian reserve. A mature oocyte may not be retrievable due to technical difficulties. Fertilization failure may be caused by sperm abnormalities or lack of penetration of the zona pellucida, an oocyte activation failure, or a defect in the oocyte
Poor embryo quality
Poor endometrial receptivity
Poor embryo transfer efficiency
Intra Cytoplasmic Sperm Injection (ICSI)
INTRODUCTION
Intracytoplasmic sperm injection (ICSI) refers to a technique in which a single sperm is injected directly into the cytoplasm of a mature oocyte. This procedure is performed as part of an in vitro fertilization (IVF) cycle, and provides an effective method for assisting fertilization in men with suboptimal semen parameters or who experienced no or low fertilization rates after conventional IVF.
This technique has consistently demonstrated higher fertilization rates and produced more embryos with higher implantation rates.
The indications for use of ICSI in conjunction with IVF have been Fertilization rates of up to 80 percent and clinical pregnancy rates of up to 45 percent are observed with ICSI, thus reducing the use of adoption or donor sperm insemination in couples with male infertility
INDICATIONS
ICSI is indicated for treatment of male factor infertility and selected types of female infertility, such as some morphologic anomalies of oocytes, limited quantities of oocytes, and anomalies of the zona pellucid. It is used in couples with previous poor fertilization or previous failed IVF cycles
ICSI is indicated for male factor infertility when success with standard IVF regimens is considered unlikely because of :
Less than 2 million motile spermatozoa per ejaculate
Antisperm antibodies thought to be causing infertility
Prior or repeated fertilization failure with standard IVF protocols
Frozen sperm limited in number and quality
Obstruction of the male reproductive tract not amenable to repair
Abnormal sperm morphology greater than 95 percent
Specific spermatozoa defects impairing spermatozoa-oocyte interaction
ICSI has also been successful in men with nonmosaic Klinefelter syndrome or long-standing azoospermia after chemotherapy; in these cases, spermatozoa are obtained from testicular biopsies.
Other potential indications for ICSI include:
HIV discordant couples
IVF involving, in vitro matured oocytes, or previously cryopreserved oocytes.
CONTRAINDICATIONS
ICSI is unlikely to improve clinical pregnancy rates in couples with unexplained infertility or low oocyte yield and advanced maternal age.
FERTILIZATION
The fertilization rate following ICSI is approximately 50 to 80 percent . Although ICSI does not guarantee fertilization, the incidence of complete fertilization failure is low and usually occurs in cycles with low oocyte yield.