Tubal ligation is a permanent voluntary form of birth control (contraception) in which a woman's Fallopian tubes are surgically cut or blocked off to prevent pregnancy.
Tubal ligation is performed in women who definitely want to prevent future pregnancies. It is frequently chosen by women who do not want more children, but who are still sexually active and potentially fertile, and want to be free of the limitations of other types of birth control. Women who should not become pregnant for health concerns or other reasons may also choose this birth control method. Tubal ligation is one of the leading methods of contraception. The typical tubal ligation patient is over age 30, is married, and has had two or three children.

Tubal ligation, or getting one's "tubes tied," refers to female sterilization, the surgery that ends a woman's ability to conceive. The operation is performed on the patient's Fallopian tubes. These tubes, which are about 10 cm long and 0.5 cm in diameter, are found on the upper outer sides of the uterus, and open into the uterus through small channels. It is within the Fallopian tube that fertilization, the joining of the egg and the sperm, takes place. During tubal ligation, the tubes are cut or blocked in order to close off the sperm's access to the egg.
Normally, tubal ligation takes about 20-30 minutes, and is performed under general anesthesia, spinal anesthesia, or local anesthesia with sedation. The surgery can be performed on either hospitalized patients within 24 hours after childbirth or on outpatients. The woman can usually leave the hospital the same day.
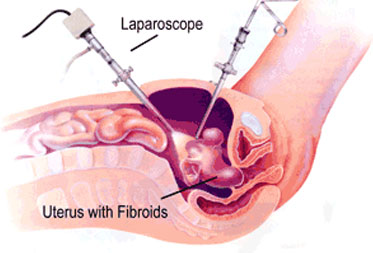
The most common surgical approaches to tubal ligation include laparoscopy and mini-laparotomy. In a laparoscopic tubal ligation, a long, thin telescope-like surgical instrument called a laparoscope is inserted into the pelvis through a small cut about 1 cm long near the navel. Carbon dioxide gas is pumped in to help move the abdominal wall to give the surgeon easier access to the tubes. Often the surgical instruments are inserted through a second incision near the pubic-hair line. An instrument may be placed through the vagina to hold the uterus in place.
In a mini-laparotomy, a 3-4 cm incision is made just above the pubic bone or under the navel. A larger incision, or laparotomy, is rarely used today. Tubal ligation can also be performed at the time of a cesarean section.
Tubal ligation costs about $2,000 when performed by a private physician, but is less expensive when performed at a family planning clinic. Most insurance plans cover treatment costs.
Preparation for tubal ligation includes patient education and counseling. Before surgery, it is important that the woman understand the permanent nature of tubal ligation, and the risks of anesthesia and surgery. Her medical history is reviewed, and a physical examination and laboratory testing are performed. The patient is not allowed to eat or drink for several hours before surgery.
After surgery, the patient is monitored for several hours before she is allowed to go home. She is instructed on care of the surgical wound, and what signs to watch for, such as fever, nausea, vomiting, faintness, or pain. These signs could indicate that complications have occurred.
While major complications are uncommon after tubal ligation, there are risks with any surgical procedure. Possible side effects include infection and bleeding. Rarely, death may occur as a complication of general anesthesia if a major blood vessel is cut. The death rate following tubal ligation is about four per 100,000 sterilizations.
After laparoscopy, the patient may experience pain in the shoulder area from the carbon dioxide used during surgery, but the technique is associated with less pain than mini-laparotomy, as well as a faster recovery period. Mini-laparotomy results in a higher incidence of pain, bleeding, bladder injury, and infection compared with laparoscopy. Patients normally feel better after three or four days of rest, and are able to resume sexual activity at that time.
Following tubal ligation, there is a low risk (less than 1%) of ectopic pregnancy. Ectopic pregnancy is a condition in which the fertilized egg implants in a place other than the uterus, usually in one of the Fallopian tubes. Ectopic pregnancies are more likely to happen in younger women, and in women whose tubes were ligated by electrocoagulation.
After having her tubes ligated, a woman does not need to use any form of birth control to avoid pregnancy. Tubal ligation is almost 100% effective for the prevention of conception. The possibility for treatment failure is very low--fewer than one in 200 women (0.4%) will become pregnant during the first year after sterilization. Failure can happen if the cut ends of the tubes grow back together; if the tube was not completely cut or blocked off; if a plastic clip or rubber band is loose or comes off; or if the woman was already pregnant at the time of surgery.
Enter your details below & we will call you back